HHS Office of Inspector General Proposes Modifications to Anti-Kickback Statute Safe Harbors to Promote Value-Based Care

Key Points:
- On Oct. 9, 2019, the U.S. Department of Health and Human (HHS) Services Office of Inspector General (OIG) has issued its proposed rule to reform the Anti-Kickback Statute’s (AKS) regulatory safe harbors to address value-based arrangements. The OIG’s proposal includes new safe harbors and modifications to existing safe harbors to protect value-based arrangements from liability under the AKS. A fact sheet describing the OIG’s proposed rule is available here.
- The goals of these reforms are to modernize existing safe harbors to the AKS and create a new exception to the Civil Monetary Penalty (CMP) law to remove potential barriers to more effective coordination and management of patient care and delivery of value-based care that improves quality of care, health outcomes and efficiency.
- The OIG specifically notes that these changes would be intended for prospective protection only and do not cover arrangements entered prior to the new proposals.
- Simultaneously, the Centers for Medicare and Medicaid Services released long-awaited proposed reforms to regulatory exceptions to the Physician Self-Referral Law (commonly known as the Stark Law), also with the goal of advancing value-based care. Akin Gump’s Client Alert on the Stark Law proposals is available here.
- Comments to the OIG’s proposal are due on Dec. 31, 2019.
Proposed New Anti-Kickback Statute Safe Harbors
In this recent rulemaking, the OIG proposes several new safe harbors for value-based arrangements as well as modifications to the existing safe harbors for personal services arrangements, electronic health records, warranties and local transportation. The OIG’s proposals reflect an effort to address innovative partnerships between different providers and other participants in the health care delivery system.
The current Anti-Kickback Statute language and safe harbors are based on a fee-for-service model of health care payment. They address fraud and abuse issues that could emerge in such an environment in which higher volume results in higher payment. But, the AKS’s provisions also unintentionally limit the ability to engage in certain value-based or outcomes-based payments that encourage innovation, better patient care and lower cost of delivery.
As the government seeks to transition from a system that pays for health care based on a fee-for-service model to a system that rewards outcomes and value, payments exchanged between parties subject to a value-based arrangement could be considered “remuneration”—i.e., a kickback—under the AKS. But, the current safe harbors do not directly apply or protect these payments from AKS liability.1
To protect value-based arrangements like these, the OIG has proposed the addition of several new safe harbors that address care coordination, value-based arrangements in which participants assume financial risk for care, patient engagement and support, and remuneration provided in connection with a CMS-sponsored payment model. In addition, the OIG also proposes to modify the existing personal services and management contracts safe harbor, warranties safe harbor and local transportation safe harbor to add flexibility with respect to care coordination and value-based arrangements.
The OIG also proposes a new safe harbor for donations of cybersecurity technology and services and modifications to the existing safe harbor for electronic health records (EHR) items and services.
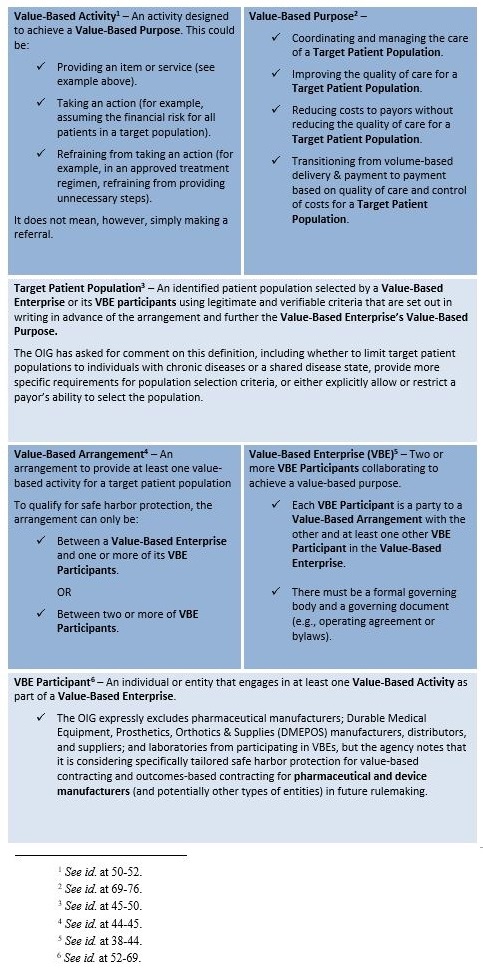
The following proposed terms are important in order to understand the scope and depth of the agency’s proposed safe harbors.
Safe Harbors for Value-Based Arrangements
In the proposed rule the OIG proposes three new safe harbors for certain remuneration exchanged between or among participants in a value-based arrangement, with greater flexibilities available to parties as they assume more downside financial risk. This “tiered” structure attempts to take into account the assumption that arrangements involving greater amounts of downside risk inherently limit incentives to order medically unnecessary or overly costly items or services.
Care Coordination Arrangements to Improve Quality, Health Outcomes and Efficiency (42 CFR § 1001.952(ee))
The OIG’s first proposed new value-based safe harbor covers “care coordination arrangements.” The safe harbor would protect from AKS liability in-kind remuneration between VBE participants intended to facilitate coordination and management of care.
The safe harbor would require the VBE to establish specific, evidence-based outcome measures against which the recipient of the remuneration will be measured. These measures would need to be grounded in legitimate, verifiable data, and be defined in a signed writing. The arrangement must be commercially reasonable and the remuneration provided must be in-kind only and used primarily to engage in value-based activities that are directly connected to the coordination and management of care of the target patient population. The safe harbor would also require the VBE to monitor and assess (at least annually) the coordination and management of care for the target patient population, progress on outcome measures, and any deficiencies in the delivery of care. Among other program safeguards, the safe harbor would also require that recipients contribute at least 15 percent of the cost of the in-kind remuneration provided.8
For example, a care coordination arrangement potentially protected by this proposed safe harbor could involve a hospital providing a behavioral health nurse to a skilled nursing facility to assist patients in transitioning after discharge from the inpatient setting.
Value-Based Arrangements With Substantial Downside Financial Risk (42 CFR § 1001.952(ff))
The OIG’s second proposed safe harbor addresses arrangements in which a VBE assumes a substantial downside financial risk from a payor for providing items and services to a target patient population. The OIG considers a VBE to be at “substantial downside financial risk” if the arrangement meets certain thresholds (i.e., shared savings with a repayment obligation to the payor of at least 40 percent of shared losses; repayment obligation to the payor under an episodic or bundled payment arrangement of at least 20 percent of any total loss; a prospectively paid population-based payment for a defined subset of the total cost of care; or a partial capitated payment from the payor reflecting a discount of at least 60 percent of the total expected fee-for-service payment for the items and services).
If the VBE assumes a substantial downside financial risk from the payor, the safe harbor protects the exchange of monetary and in-kind remuneration between the VBE and a VBE participant that meaningfully shares in the VBE’s downside financial risk. (“Meaningfully shares” means that the VBE participant assumes a certain percentage of the VBE’s overall financial risk, is subject to a partial or full capitation payment or similar payment methodology; or, in the case of a physician, meets the recently proposed Stark Law exception for value-based arrangements with meaningful downside financial risk.)
The OIG also proposes certain program integrity requirements and controls (i.e. arrangement must be set forth in a signed writing, cannot condition remuneration on patient or business referrals outside the arrangement, etc.) for these arrangements. In addition, the remuneration provided under any protected arrangement must be used primarily to engage in value-based activities that are directly connected to the items and services for which the VBE is at substantial downside financial risk.9
For example, a VBE is at substantial downside financial risk through an agreement with a payor to assume a percentage of shared losses for items and services provided in connection with hip replacements to the target patient population. Remuneration provided by the VBE to a VBE participant would potentially be protected as long as the VBE participant primarily uses the remuneration to engage in value-based activities that have a direct connection to the items and services provided to patients in the target population.
Value-Based Arrangements with Full Financial Risk (§ 1001.952(gg))
The OIG’s third proposed safe harbor addresses arrangements in which a VBE assumes the full financial risk from a payor for providing items and services for a target patient population. The OIG notes that this safe harbor imposes the fewest restrictions and allows VBEs the greatest ability to innovate on care coordination.
The OIG proposes that a VBE would be at “full financial risk” for the cost of care of a target patient population if the VBE is financially responsible for the cost of all items and services covered by the applicable payor for each patient in the target patient population and is prospectively paid by the applicable payor.
If the VBE assumes the full financial risk, the safe harbor would protect the exchange of monetary and in-kind remuneration between a VBE and a VBE participant. It does not require that the VBE participant “meaningfully share” in the VBE’s downside risk. In addition, the OIG proposes the VBE meet certain additional requirements designed to promote transparency and accountability and other program integrity requirements, such as requiring the arrangement be documented in writing and signed by the parties, the term of the arrangement be for at least one year, and prohibiting VBE participants from claiming additional payment for item or service covered under the arrangement. Similar to the substantial downside financial risk safe harbor, the remuneration exchanged must be used primarily to engage in value-based activities and directly connected to one or more of the VBE’s value-based purposes.10
A VBE would be at full financial risk if it received a prospective, capitated payment for all items and services covered by Medicare Parts A and B for a target patient population.
Other Proposed Safe Harbors
Arrangements for Patient Engagement and Support (42 CFR § 1001.952(hh))
The OIG’s fourth proposed safe harbor protects from AKS liability the provision of in-kind patient engagement tools and supports to improve quality, health outcomes and efficiency.
Examples: Providing supports that improve patients’ safety at home or during care transitions or that allow providers to communicate more efficiently and effectively with patients and to monitor care.
To qualify for safe harbor protection, the VBE participant must provide an in-kind preventive item, good or service (such as health related technology, patient health related monitoring tools and services, or supports and services). The item, good or service must have a direct connection to the coordination and management of care of the target patient population. Under the proposal, these tools must be furnished directly to the patient by a VBE participant, and no individual or entity outside of the applicable VBE can contribute to the provision of the patient engagement tool or support.
The OIG also proposes several program integrity requirements, including a ban on gift cards, cash or cash equivalents. Further, the OIG requires that these tools and supports must advance adherence to a treatment or drug regimen, follow-up care plan, disease or condition management determined by the patient’s provider. The OIG also indicates that the aggregate retail value of tools and supports provided to a patient cannot exceed $500 annually, unless based on a good faith, individualized determination of the patient’s financial need.11
CMS-Sponsored Models and Patient Incentives (§ 1001.952(ii))
The OIG’s proposed rulemaking also seeks to advance the government’s current initiatives to operate and test new alternative payment models and encourage shared savings. The OIG issued a proposed new safe harbor that would protect remuneration between parties to arrangements (e.g., distribution of capitated payments, shared savings or loss distributions) under an alternative payment model or other initiative being tested or expanded by the CMS Innovation Center and the Medicare Shared Savings Program. It would also allow remuneration in the form of incentives provided by CMS alternative payment model participants to patients covered by the model.12
Cybersecurity Technology and Services (§ 1001.952(jj))
Citing the importance of cybersecurity to allowing health care industry participants to collaborate and share data, the OIG proposes a new safe harbor to protect donations of certain cybersecurity technology and related services. The safe harbor would protect from AKS liability the donation of cybersecurity technologies and a broad range of services supporting those technologies (e.g., installation, training, business continuity and data recovery services, monitoring cybersecurity, risk assessments, etc.).
Any donated cybersecurity technology and services must be documented in writing and cannot be conditioned on referrals generated between the parties. The safe harbor would not require recipients to contribute to the cost of the services. The safe harbor would also not specify who may donate or receive this remuneration, and may include patients as recipients.
The OIG makes clear that its proposal does not include hardware—only software and related services—as the agency views donations of “multifunctional” hardware as posing a higher risk of constituting a disguised payment for referrals. The OIG does, however, ask whether it should permit hardware donations in limited circumstances if determined to be necessary as part of a cybersecurity risk assessment.13
Proposed Modifications to Existing Safe Harbors
In addition to proposing new safe harbors, the OIG also recommends revisions to existing AKS safe harbors to address value-based arrangements. This includes revisions to the personal services and management contracts safe harbor that would modernize its technical requirements and would permit outcomes-based payments for delivering higher quality patient care. The OIG proposes an expansion of the warranties safe harbor that would allow companies to offer warranty protections for a wider range of items and services.
Personal Services and Management Contracts Safe Harbor (§ 1001.952(d))
The OIG proposed to revise this safe harbor to modify several technical requirements for safe harbor compliance. This includes eliminating the requirement that compensation must be set in advance, requiring instead that the methodology for determining compensation be set in advance. The OIG also proposes to allow greater flexibility for part-time arrangements by eliminating the requirement that the parties specify the exact schedule, length and associated charges part-time arrangements. These are significant changes that provide greater flexibility for complying with the safe harbor.14
The OIG also proposed add a new provision to the safe harbor to protect certain outcomes-based payments from AKS liability. The OIG defines outcomes-based payments as payments rewarding the recipient for improving patient or population health by achieving outcome measure(s) that coordinate care across care settings or reduce a payer’s costs while improving or maintaining quality of care for patients.
Notably, the OIG explicitly excludes payments made directly or indirectly, by a pharmaceutical manufacturer; a manufacturer, distributor, or supplier of DMEPOS; or a laboratory from the safe harbor’s protection and questions whether other entities (medical device makers, pharmacy benefit managers, pharmacies and others) should also be excluded from protection.
The new proposed provision includes a number of safeguards, including requiring evidence-based outcome measures as the basis for a payment and rebasing outcomes measures periodically.15
Warranties (§ 1001.952(g))
The OIG proposes to modify its safe harbor protecting certain warranty payments from AKS liability. In particular, the OIG proposes to protect the payment or exchange of anything of value under a bundled warranty for one or more items and related services when certain conditions are met. This change expands the current warranties safe harbor, which only protects warranties offered on a single product. The goal is to allow manufacturers to offer more innovative protections for purchasers based not only on repairing and replacing defective products, but also covering the costs of related services associated with the item.
If a manufacturer or supplier offers a warranty for more than one item or a bundle of items and related services, according to the OIG’s proposal, the items and services subject to the warranty must be reimbursed by the same Federal health care program and in the same Federal health care program payment. This means, for example, the same Part A Medicare Severity-Diagnosis Related Group (DRG) payment, the same Medicare Part B ambulatory payment classification payment or the same Medicaid managed care payment.16
Electronic Health Records (EHR) Items and Services (§ 1001.952(y))
The OIG proposes to modify its existing safe harbor protecting donations of electronic health records software, updating the rule’s requirements relating to interoperability and information blocking (i.e., providing technology that may facilitate care coordination in the VBE but that prevents the exchange of electronic health information with other providers to lock-in referrals between VBE providers), removing the sunset provision and modifying certain definitions. The OIG is also considering modifying or eliminating the current requirement that recipients of EHR technology contribute at least 15 percent of the technology’s costs.17
Local Transportation Safe Harbor (§ 1001.952(bb))
The OIG also proposed to expand the AKS safe harbor for local transportation, noting that the distance some patients travel to a health care provider can be a barrier to better care. The provision of certain no-charge transportation is not considered “remuneration” subject to AKS liability under the existing safe harbor. The OIG proposes to expand the permitted distance that residents of rural areas may be transported to 75 miles (currently, 50 miles). The OIG also proposes to eliminate the mileage limits for transportation of patients discharged from inpatient facilities to their residence or a different residence of their choosing. Last, the OIG clarifies that it views the use of ride share services as analogous to the use of taxis, which are permitted under the safe harbor.18
Other Updates
In addition to the new and modified safe harbors described above, the OIG also proposes to codify two statutory provisions that protect the provision of items and services directly to Medicare beneficiaries.
Accountable Care Organization (ACO) Beneficiary Incentive Programs (§ 1001.952(kk)).
The OIG proposed to codify the statutory exception to the definition of “remuneration” related to ACO Beneficiary Incentive Programs under the Medicare Shared Savings Program. The Medicare Shared Savings Program encourages providers to form ACOs that agree to be responsible for the cost, quality and experience of care for an assigned Medicare beneficiary population. The purpose is to promote accountability and to foster better coordination of care and quality of care for Medicare beneficiaries. An ACO that achieves quality and cost savings goals can share in a percentage of the savings with Medicare.
As part of these efforts, ACOs can operate beneficiary incentive programs that encourage Medicare beneficiaries to obtain medically necessary primary care services. For example, an ACO might incentivize a Medicare beneficiary to attend a visit with his or her primary care provider by giving out a gift card for each visit attended. The OIG proposes to add a new safe harbor that would protect these payments (currently capped at $20 for each qualifying service received) from AKS liability, as required by recent statutory revisions.19
Telehealth for In-Home Dialysis: Proposed Amendment to Beneficiary Inducements CMP Exception (42 C.F.R. § 1003.110).
Finally, the OIG proposes to codify a statutory exception to the beneficiary inducements CMP rule that would protect the transfer of certain technology to in-home dialysis patients. Similar to the AKS, the beneficiary inducements CMP statute criminalizes the offering of remuneration to a program beneficiary to influence the beneficiary selection of a particular provider.
The OIG’s proposal provides that “remuneration” for purposes of this rule does not include the provision of telehealth technologies by a provider to an individual with end stage renal disease who is receiving home dialysis. The rulemaking also includes additional program integrity restrictions (e.g., the technology cannot be offered as part of an advertisement).20
1 Revisions to Safe Harbors under the Anti-Kickback Statute, and Civil Monetary Penalty Rules Regarding Beneficiary Inducements 8-10, https://www.hhs.gov/sites/default/files/oig-nprm.pdf (proposed Oct. 9, 2019) (to be published in the Federal Register).
2 See id. at 50-52.
3 See id. at 69-76.
4 See id. at 45-50.
5 See id. at 44-45.
6 See id. at 38-44.
7 See id. at 52-69.
8 See id. at 76-120.
9 See id. at 120-35.
10 See id. at 135-47.
11 See id. at 147-92.
12 See id. at 192-210.
13 See id. at 211-43.
14 See id. at 267-70.
15 See id. at 270-87.
16 See id. at 287-300.
17 See id. at 243-67
18 See id. at 300-10.
19 See id. at 310-15.
20 See id. at 316-29.
Attachments
Authors


{kind=link}